Microwave ablation of two deeply situated liver tumours in segments IV and VII. Interoperative ablation margin control assessed the ablation volume and confirmed the need for reablation. A CT-MRI fusion was performed for the 'invisible' segment VII lesion on CT. Percutaneous microwave ablation was selected as the safer, non-invasive treatment option over surgical resection.
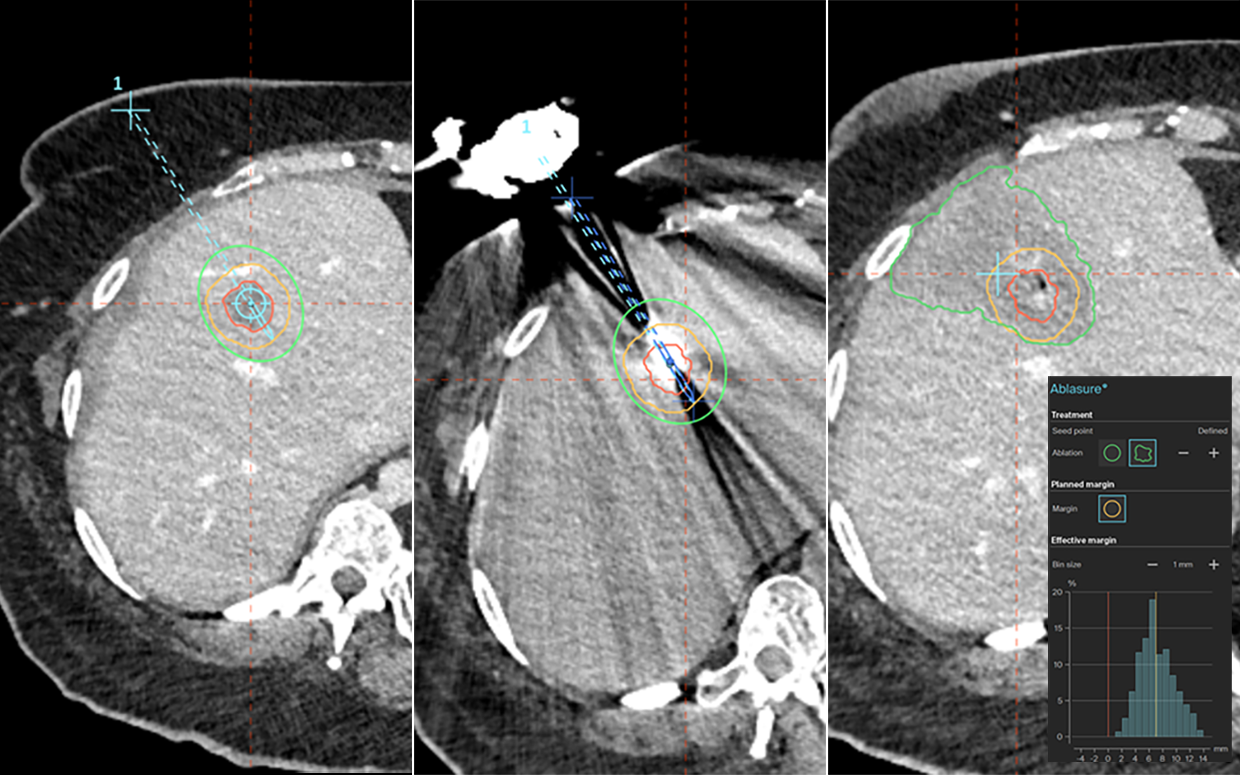
1. Trajectory plan | Needle verification | Automatic ablation zone segmentation + AblaSure screen
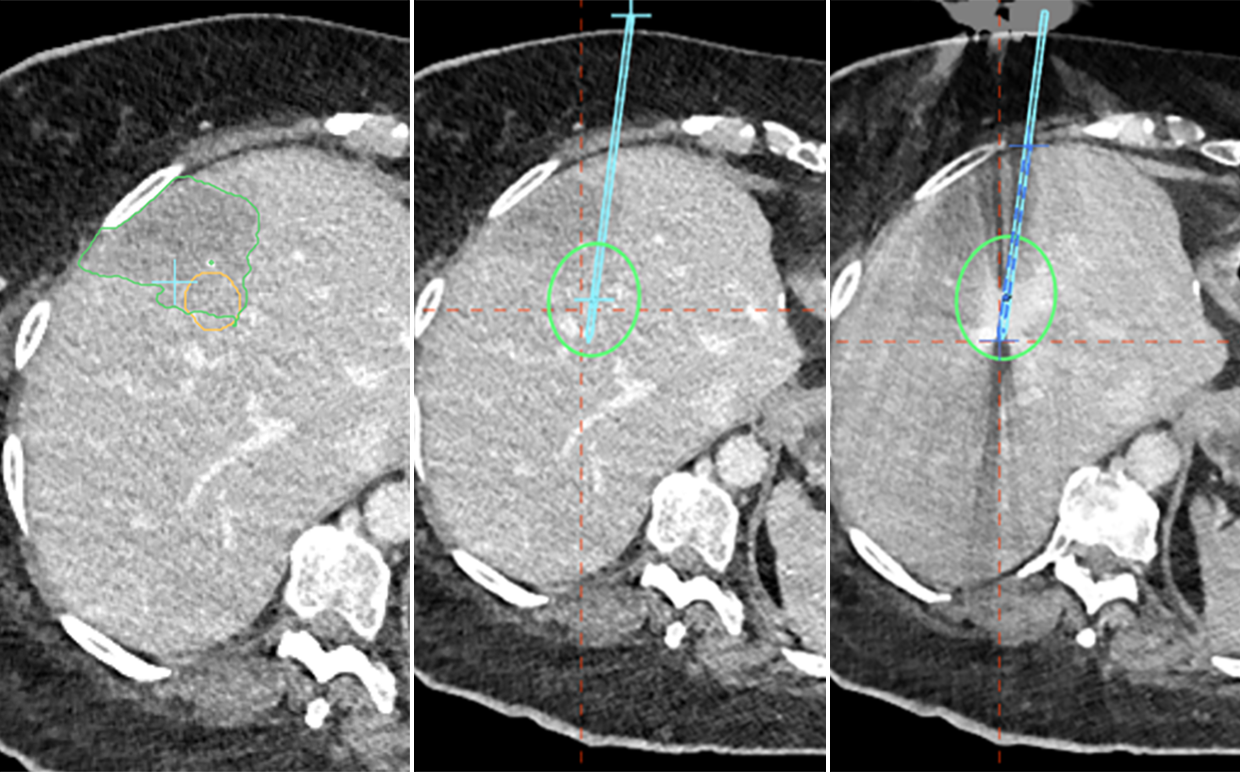
2. Under-coverage of clinical margin confirmed | Re-ablation trajectory plan | Re-ablation needle verification
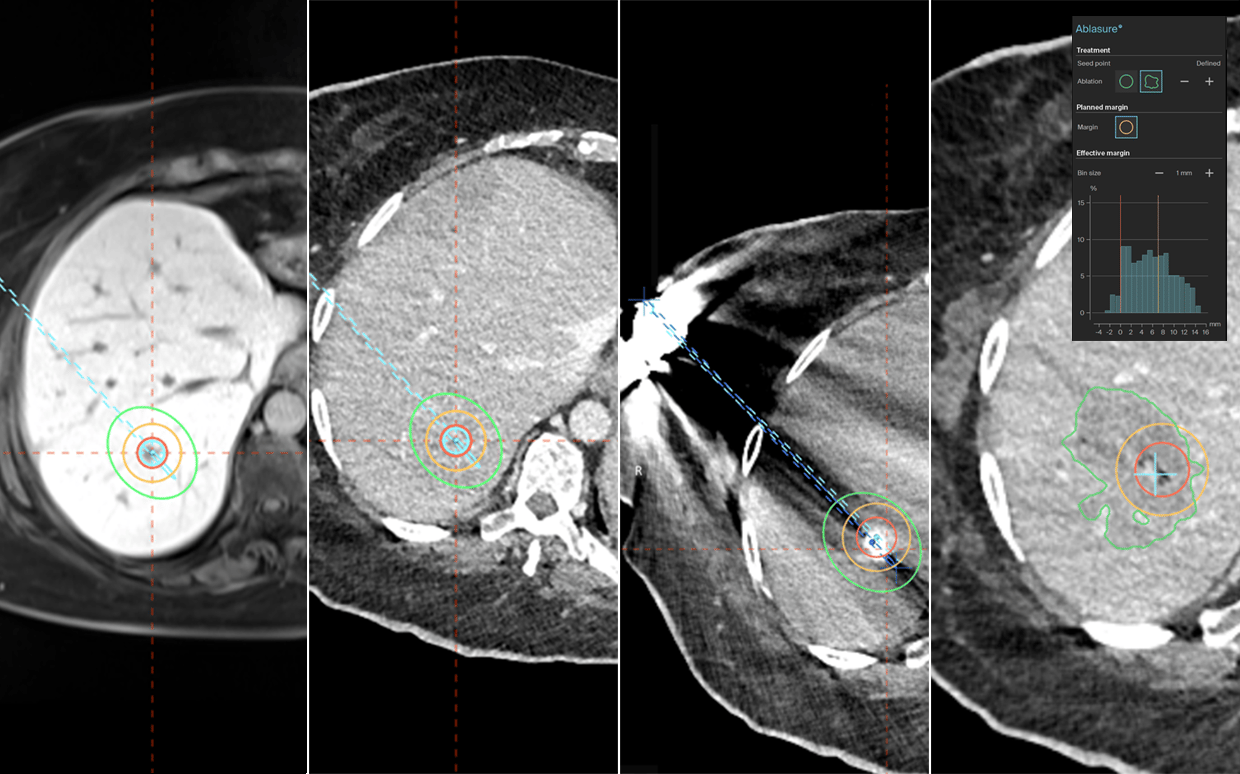
Lesion visible on MRI | CT-MRI fusion plan | Needle verification | Automatic ablation zone segmentation + AblaSure screen
Name: Dr Shaheen Noorani
Institution: Basingstoke and North Hampshire NHS Trust (United Kingdom)
Patient age and sex: 53 female
Initial condition:
- Patient presented with a metastatic colorectal cancer lesion in segment VII of the liver
- Metastatic lesion was resected which resulted in sepsis and the patient required recovery time of six months
- Residual lesion was still in situ and developed further metastasis
- The patient then underwent chemotherapy, resulting in a good response and evident tumour reduction
- Ablation of the two deeply situated metastatic lesions (segment VII and segment IV) and subsequently, liver wedge resection with removal of the remaining lesions was planned
Treatment:
- The patient was under GA and respiratory motion control, enabled using apnea during scanning and needle insertion
- MWA ablation of the segment IV lesion was planned with CAS-One IR and after navigated needle placement, the 4mm lateral needle displacement was compensated for by increasing the time of ablation to subsequently increase the ablation zone
- Post ablation analysis using AblaSure confirmed a slight under-ablation of the clinical margin, and the decision was made to re-ablate
- A CT-MRI fusion with CAS-One IR was performed for the invisible lesion on CT, in segment VII. The needle placement was accepted and AblaSure analysis showed complete ablation of the tumour
Conclusion:
- Post ablation assessment allowed for concise analysis of the ablation zone, clearly confirming the need for re-ablation of the segment IV lesion
- The CT-MRI fusion with CAS-One IR was essential to accurately locate the invisible segment VII lesion
- Ablation of both lesions was successful, and the patient was discharged the following day
