Ablation of a solitary lesion high up in the liver dome with an inferior-to-superior oblique trajectory using a non transthoracic approach. Quality Ablation with CAS-One IR helped increase the accuracy of the needle placement and safety for the patient during the procedure.
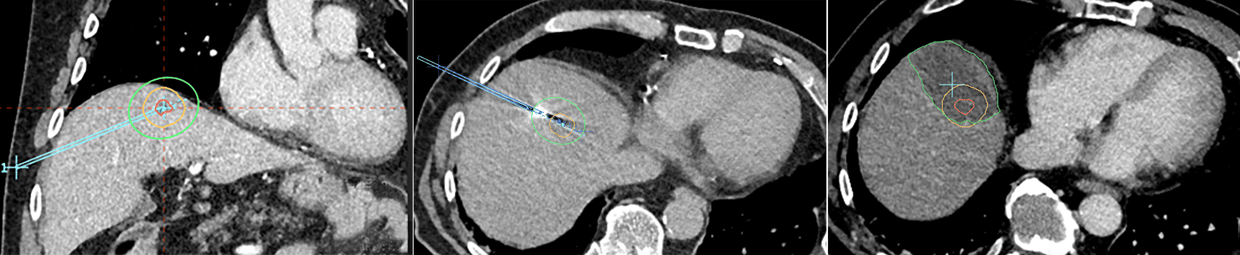
Left: Coronal planning scan showing lesion in segment VIII in the liver dome planning of segmented tumour with 8mm margin
Middle: Needle validation scan. Burn time was 4 min
Right: Tumour (red) and the majority of the clinical margin (yellow) are covered by the ablation volume (green)
Middle: Needle validation scan. Burn time was 4 min
Right: Tumour (red) and the majority of the clinical margin (yellow) are covered by the ablation volume (green)
Name: Dr. Shaheen Dixon
Institution: Basingstoke and North Hampshire Hospital, UK
Patient age and sex: 80 years, male
Initial condition:
- Carer for wife and son
- Peripheral vascular disease and stenosis of the SMA and coeliac trunk
- 2002: Coronary artery bypass grafting
- 2012: Right hemicolectomy
- 2018: Transurethral resection for transitional cell carcinoma (TCC) blatter (G1pTa)
- 2019: Anterior resection for colorectal cancer (T3N0)
- 06/2021: PET, CT and MRI demonstrates solitary liver metastasis in seg VIII high up in the liver dome, size 13 x 10 x 12mm
- 09/2021: Freehand ablation attempt failed due to the significant breathing motion causing movement of the liver, despite anaesthetic breath hold. This posed a high risk for pneumothorax of the right lung. Several loads of contrast were administered and repeated scans taken to try and achieve the ablation.The last procedure took a total of four hours, then was abandoned. The patient went into urinary retention and was discharged 2 days later
- CAS-One IR allowed the insertion of the needle with an inferior-to-superior oblique trajectory avoiding a transthoracic approach, whilst increasing accuracy and safety during the procedure for the patient
Treatment:
- Non-transthoracic, oblique trajectory planned and needle for microwave ablation inserted
- Ablasure showed complete ablation of the tumour but slight under ablation of the 8mm clinical margin
- Total procedure time from planning scan to ablation was one hour, showcasing a quick learning curve of the physician since the recent introduction of Quality Ablation
- Patient recovered from procedure and discharged the following morning
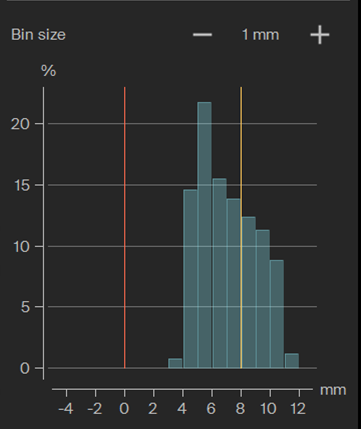
Quantative margin assessment using AblaSure shows complete ablation of the tumour and the majority of the 8mm clinical margin
Conclusion by Dr. Shaheen Dixon:
- One advantage of CAS-One IR is that it allows planning of difficult trajectories in 3D. In this case it was possible to achieve the ablation without traversing the lung, reducing the chance of the patient having a pneumothorax
- Reduction of radiation dose to the patient and staff. The contrast runs required are minimal and therefore reduces the amount of contrast needed
- The segmentation functionality of the system allows clear identification of ablation margins, which in turn leads to more confidence, that the lesion was ablated with good technical success rather than the visual eyeballing and estimating it. In this case it was extremely important to achieve a good ablation zone on this patient due to his comorbidities and the fact that he is the sole carer for his wife and son
- The system is overall easy to use and can be adapted into the workflow easily with practice. We are confident that this will increase our accuracy of A0 ablations, increase the types of ablations we can do and reduce overall re-ablation rates
