A 66-year-old male with Hepatitis C-related cirrhosis and HCC presented for CAS-One IR guided microwave ablation of a segment IVa lesion. He had previously undergone right hepatectomy with clear margins in November 2023. A small 4mm nodule in segment IVa was detected on surveillance imaging and monitored closely, growing to 6mm at three months and 8mm at the subsequent three-month follow-up. Progression was confirmed on CT in February 2026. The case was reviewed at the multidisciplinary team meeting, where the decision was made to proceed with CAS-One IR guided microwave ablation due to the challenging position close to the heart.
Name: Dr. Mudassir Rashid
Institution: Gold Coast University Hospital
Patient age and sex: 66, Male
-
Hepatitis C-related cirrhosis and HCC; Hepatitis C cured 2019
-
November 2023: right hepatectomy for 35mm segment VII HCC with clear margins
-
June 2024: 44mm extra-hepatic porto-caval lymph node on MRI; commenced on atezolizumab plus bevacizumab
-
Surveillance imaging identified a 4mm segment IVa nodule, which grew to 6mm and subsequently 8mm on consecutive three-month follow-up scans
-
CT February 2026 confirmed progression of the segment IVa lesion
-
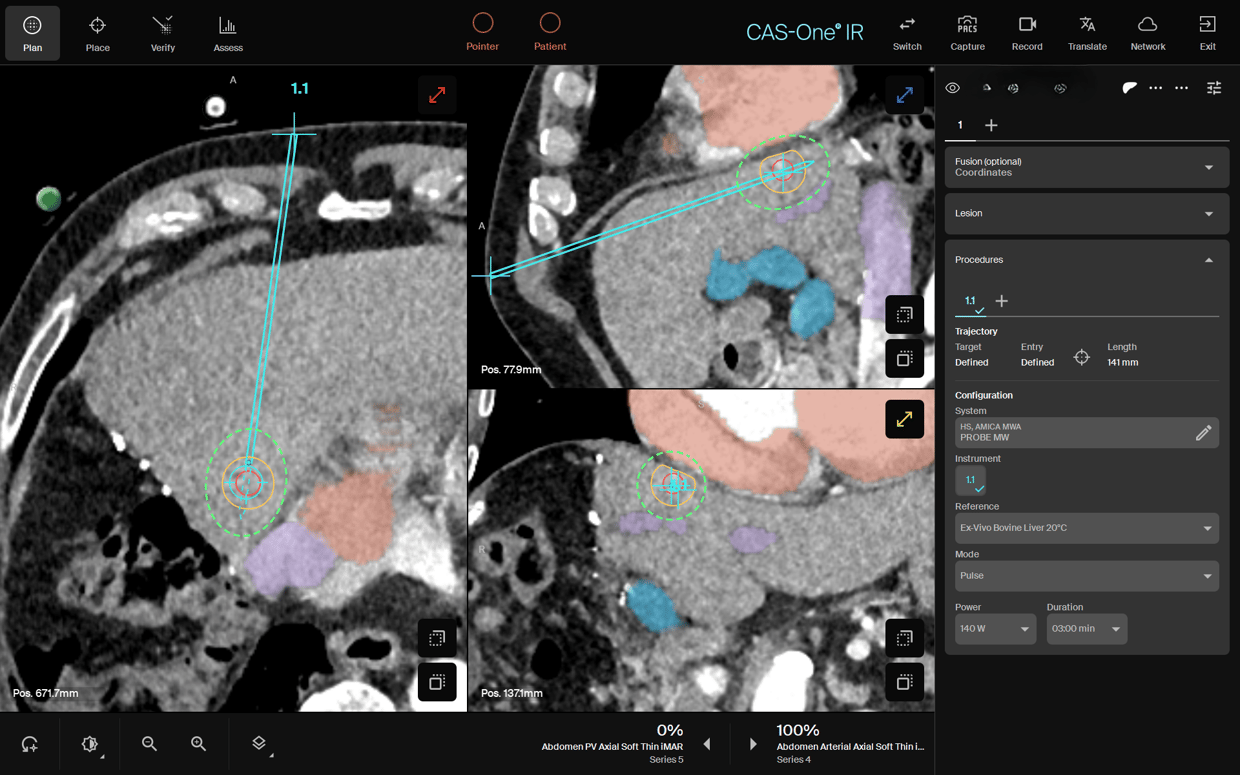
Case discussed at MDT; surgical re-resection declined given previous right hepatectomy. Radiation oncology consulted and held in reserve. Decision made to proceed with MWA using CAS-One IR given anatomical proximity to the heart superiorly and portal vein inferiorly
-
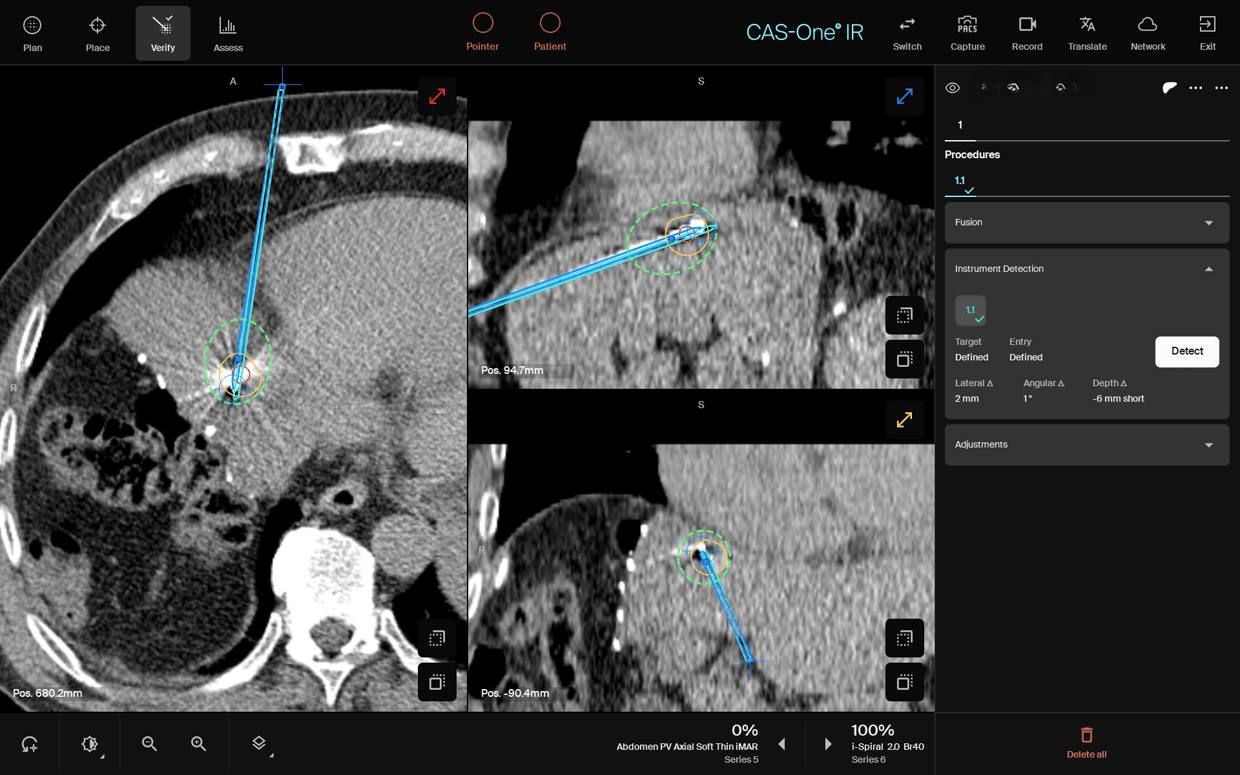
Procedure performed under general anaesthesia with endotracheal intubation and complete neuromuscular paralysis; long breath holds used throughout to optimise targeting accuracy
-
All critical anatomical relationships: cardiac border superiorly, portal vein inferiorly, were accounted for during planning
-
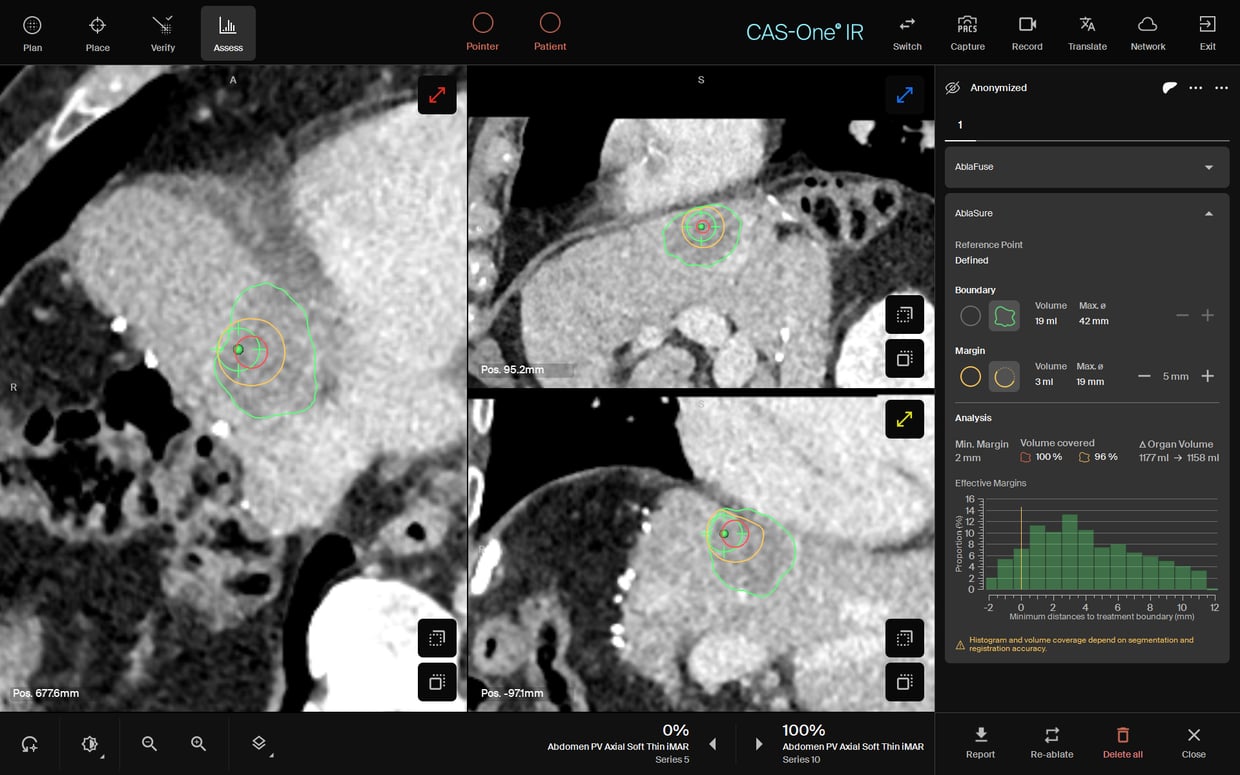
AblaSure® confirmed an 8mm ablative margin circumferentially around the lesion
-
The patient tolerated the procedure well
- Routine surveillance imaging planned at three-monthly intervals
- Patient to recommence atezolizumab plus bevacizumab two weeks post procedure
Dr. Mudassir Rashid said of the case: "Tumors like this one, close to the heart before we had CAS-One IR would have been unlikely ablation candidates, or at the very least would have taken 4+ hours. With CAS-One IR, we were able to plan, place, and ablate in about 45 minutes, and the ablation showed excellent tumor and margin coverage. We continute to have confidence in the device in situations like this where the lesion is close to a critical structure"
